8 - Associations Between Early Fluid Resuscitation, SIRS Status, and BUN Changes in Acute Pancreatitis: Real World Results From the APPRENTICE Consortium
Award: ACG Outstanding Research Award in the Biliary/Pancreas Category (Trainee)
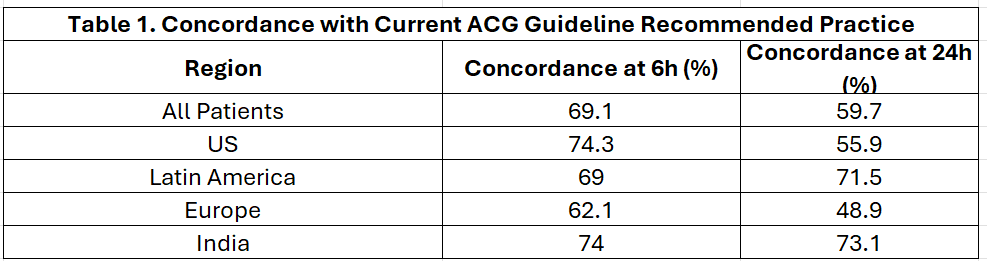
Daniel Marino, MD, MBA1, Stacey Culp, PhD2, Peter Lee, MBBCh2, Jordan Burlen, MD3, Raj Shah, MD3, Tamas Gonda, MD1, Georgios I. Papachristou, MD, PhD2 1NYU Langone Health, New York, NY; 2The Ohio State University Wexner Medical Center, Columbus, OH; 3College of Medicine, The Ohio State University, Columbus, OH Introduction: The severity of acute pancreatitis is difficult to prognosticate. New onset or persistent systemic inflammatory response syndrome (SIRS) and increase in blood urea nitrogen (BUN) have been associated with severe disease. We investigated the relationships between fluid resuscitation approaches, SIRS, and BUN as well as characterized the adherence to the most recent ACG guidelines to determine if fluid volumes correlated with known predictors of severity. Methods: Patients admitted with a diagnosis of AP were prospectively enrolled from 22 international sites from 4 different continents between 2015 and 2018. Fluid administration rates and volumes at 6 and 24 hours from presentation were collected. BUN and SIRS status were also assessed on presentation and at 24 hours. Logistic regression adjusted for region was used to assess associations between fluid administration, BUN, and SIRS. Adherence to moderately aggressive fluid resuscitation per current ACG guidelines was defined as fluid rate >1.5mL/kg/hr. Results: At first 6 hours from presentation (n=950), patients received an average of 1,173 mL of fluids with a rate of 2.59 mL/kg/hr. At 24 hours (n=957), patients received an average of 3,251 mL of fluid with a rate of 1.81 mL/kg/hr. Between admission and 24 hours, 31.3% of patients demonstrated new-onset or persistent SIRS (9% new, 22% persistent) and 32% of patients had an increase in BUN levels. Every 1 mL/kg/hr increase in fluid rate at 6 and 24 hours was associated with increased odds of persistent/new SIRS (OR 1.327, 95% CI: 1.207–1.460; OR 1.294, 95% CI: 1.091–1.536, respectively). Increased fluid rates were associated with decreased odds of BUN rise at 24 hours (OR 0.876 at 6 hours, OR 0.829 at 24 hours). Mean change in BUN was -1.5 mg/dL in patients without SIRS vs. +0.7 mg/dL in those with new/persistent SIRS (p = 0.005). Discussion: Higher early rates of fluids were associated with an increased risk of new or persistent SIRS. This likely reflects that more fluids administered to patients assessed as higher risk for severe AP by treating physicians. It appears that adequate fluid resuscitation during the first 24 hours can prevent BUN elevation but does not prevent new or persistent SIRS.
Figure: Table 1. Concordance with Current ACG Guideline Recommended Practice
Disclosures: Daniel Marino indicated no relevant financial relationships. Stacey Culp indicated no relevant financial relationships. Peter Lee indicated no relevant financial relationships. Jordan Burlen indicated no relevant financial relationships. Raj Shah indicated no relevant financial relationships. Tamas Gonda indicated no relevant financial relationships. Georgios Papachristou: AbbVie – Grant/Research Support.
Daniel Marino, MD, MBA1, Stacey Culp, PhD2, Peter Lee, MBBCh2, Jordan Burlen, MD3, Raj Shah, MD3, Tamas Gonda, MD1, Georgios I. Papachristou, MD, PhD2, 8, Associations Between Early Fluid Resuscitation, SIRS Status, and BUN Changes in Acute Pancreatitis: Real World Results From the APPRENTICE Consortium, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.