35 - Early versus Delayed Cholecystectomy in Patients Admitted for Choledocholithiasis: Impact on Biliary Complications and Role of Sphincterotomy or Stenting
Jessica El Halabi, MD, MBI, Arpita Jajoo, MD, Yana Cai, MD, Aditya Chandrashekar, MBBS, Jianing Li, MD, Alistar Kent, MD, Venkata Akshintala, MD, PhD The Johns Hopkins Hospital, Baltimore, MD Introduction: Choledocholithiasis complicates up to 20% of symptomatic cholelithiasis cases and is typically managed with endoscopic retrograde pancreatography (ERCP) followed by cholecystectomy. Although early cholecystectomy (EC) is guideline-recommended, delays are common due to clinical and logistical barriers. We aimed to examine biliary complication rates in EC versus delayed cholecystectomy (DC), the role of ERCP with sphincterotomy or stent placement, and barriers to timely surgery. Methods: We conducted a retrospective cohort study of adults admitted with choledocholithiasis in a large healthcare system from 2005–2023 with ≥12 months follow-up. EC was defined as surgery during the index admission, while DC was defined as post-discharge cholecystectomy or if cholecystectomy was not performed. Primary outcomes were biliary complications, readmissions, and mortality within one year. Secondary outcomes included biliary complications in ERCP with and without sphincterotomy or stent placement, and reasons for DC. All study outcomes were adjudicated via independent chart review. A Sankey plot illustrated biliary complications over time in EC vs. DC groups. Univariable regression was used to assess whether ERCP with sphincterotomy or stent placement reduced biliary complications. Results: We included 507 patients (median age 59, 59.4% female), among which 265 (52.3%) underwent EC and 242 (47.7%) underwent DC. Biliary complications occurred in 23% of DC vs. 0.8% of EC patients (p< 0.001). Among DC patients, 15.5% developed complications within 3 months, 6.5% by 6 months, and 1% by 12 months (Figure). Neither ERCP with sphincterotomy (26% vs. 21%, p=0.74) nor stenting (25% vs. 27%, p=0.81) significantly reduced biliary complication rates in patients that had DC. The top reasons for DC included high surgical risk (27.3%), concurrent biliary pathology (19.2%), and physician preference (14%). Discussion: Delayed cholecystectomy is associated with a >17-fold increase in biliary complications, most occurring within 90 days of discharge. Neither sphincterotomy nor stenting during ERCP mitigates this risk. Common reasons for DC include high surgical risk, concurrent pathology, and physician preference. EC during the index admission remains the most reliable strategy to reduce recurrent events. These findings suggest an opportunity for systemic interventions, including prioritization algorithms and better perioperative coordination, to address preventable delays.
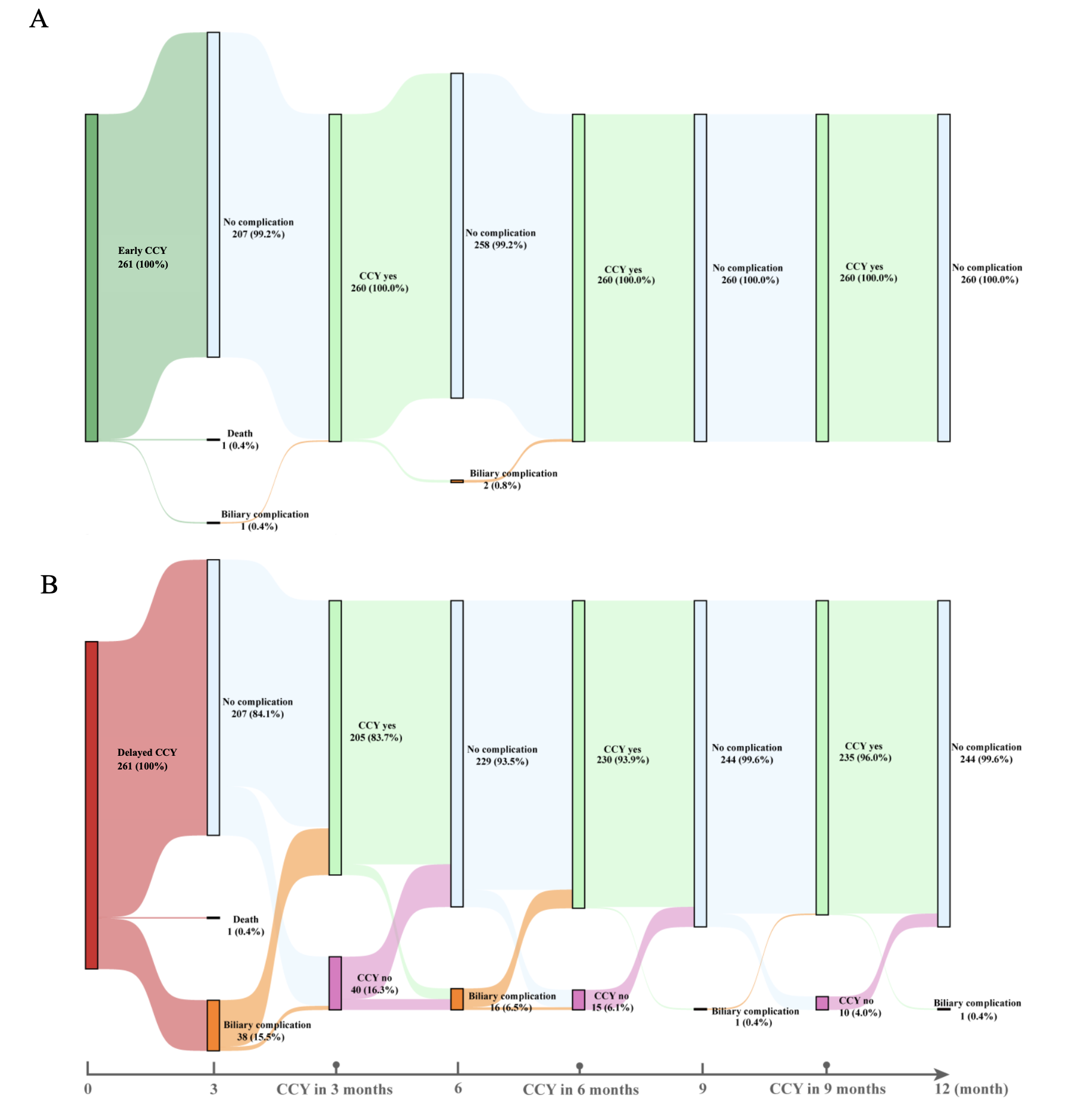
Figure: Sankey plots show biliary complications at 3-month intervals for patients undergoing early (top) vs. delayed (bottom) cholecystectomy and demonstrates the percentage of patients who underwent cholecystectomy at different intervals in the delayed cholecystectomy group. Early cholecystectomy was associated with minimal biliary complications (0.8%). In contrast, delayed surgery led to higher complication rates (23%), particularly in the first 6 months post-admission. Almost 96% had cholecystectomy within 12 months after discharge.
Disclosures: Jessica El Halabi indicated no relevant financial relationships. Arpita Jajoo indicated no relevant financial relationships. Yana Cai indicated no relevant financial relationships. Aditya Chandrashekar indicated no relevant financial relationships. Jianing Li indicated no relevant financial relationships. Alistar Kent indicated no relevant financial relationships. Venkata Akshintala indicated no relevant financial relationships.
Jessica El Halabi, MD, MBI, Arpita Jajoo, MD, Yana Cai, MD, Aditya Chandrashekar, MBBS, Jianing Li, MD, Alistar Kent, MD, Venkata Akshintala, MD, PhD, 35, Early versus Delayed Cholecystectomy in Patients Admitted for Choledocholithiasis: Impact on Biliary Complications and Role of Sphincterotomy or Stenting, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.