73 - Efficacy and Safety of Obefazimod in Patients With Moderately to Severely Active Ulcerative Colitis: Results From Two, Phase 3, Randomised, Double-Blind, Placebo-Controlled, 8-Week Induction Trials (ABTECT 1 & 2) (Late-Breaking Abstract)
Bruce E. Sands, MD, FACG1, Silvio Danese, MD2, Laurent Peyrin-Biroulet, MD3, Marla C. Dubinsky, MD4, Tadakazu Hisamatsu, MD5, Herbert Tilg, MD6, Raja Atreya, MD7, Alessandro Armuzzi, MD8, Xavier Treton, MD9, Filip Baert, MD10, Ursula Seidler, MD11, Fabio Cataldi, MD12, Doug Jacobstein, MD12, Christopher J. Rabbat, PhD12, Kejia Shan, MS12, George Aaron Duvall, MD13, Britta Siegmund, MD14, Parambir S. Dulai, MD15, David T. Rubin, MD, FACG16, Séverine Vermeire, MD171Icahn School of Medicine at Mount Sinai, New York, NY; 2Gastroenterology and Endoscopy IRCCS Ospedale San Raffaele, Italy, Milan, Lombardia, Italy; 3INFINY Institute, INSERM NGERE, CHRU Nancy, Vandœuvre-lès-Nancy, Lorraine, France; 4Mount Sinai Kravis Children’s Hospital, New York, USA, New York, NY; 5 Kyorin University School of Medicine, Tokyo, Tokyo, Japan; 6 University Innsbruck, Innsbruck, Tirol, Austria; 7University Hospital Erlangen, Erlangen, Bayern, Germany; 8IRCCS Humanitas Research Hospital, Milan, Lombardia, Italy; 9Groupe Hospitalier Prive Ambroise Pare – Hartmann, Institut des MICI, Neuilly sur Seine, Ile-de-France, France; 10AZ Delta, Roeselare, West-Vlaanderen, Belgium; 11Medizinische Hochschule Hannover, Hannover, Sachsen, Germany; 12Abivax, Paris, Ile-de-France, France; 13Tyler Research Institute, LLC, Tyler, TX; 14Charité Universitätsmedizin Berlin, Berlin, Germany; 15Feinberg School of Medicine Northwestern University - Chicago, IL; 16University of Chicago Medicine, Chicago, IL; 17University Hospitals Leuven, Leuven, Oost-Vlaanderen, Belgium Introduction: Obefazimod (Obe), an oral, once-daily (QD), small molecule which enhances expression of microRNA-124 was studied in patients (pts) with moderately to severely active ulcerative colitis (UC) in Phase 2 induction trials and in subsequent open-label maintenance studies1. Here we report the efficacy and safety of two Phase 3, 8-week induction trials in adult pts with UC from ABTECT-1 [NCT05507203] and ABTECT-2 [NCT05507216]. Methods: The randomized, double-blind, placebo-controlled ABTECT trials enrolled pts with UC (MMS ≥ 5 with RBS ≥ 1 and centrally read endoscopic score ≥2) who had inadequate response, loss of response, or intolerance to at least one prior therapy (with no upper limit), including corticosteroids, immunosuppressants, biologics, S1P receptor modulators and/or JAK inhibitors. Pts were randomized 2:1:1 to Obe 50 mg QD (Obe-50), Obe 25 mg QD (Obe-25) or placebo (PBO) for 8 weeks. The primary endpoint was clinical remission (per MMS) and key secondary endpoints included clinical response, endoscopic improvement, and histo-endoscopic mucosal improvement.
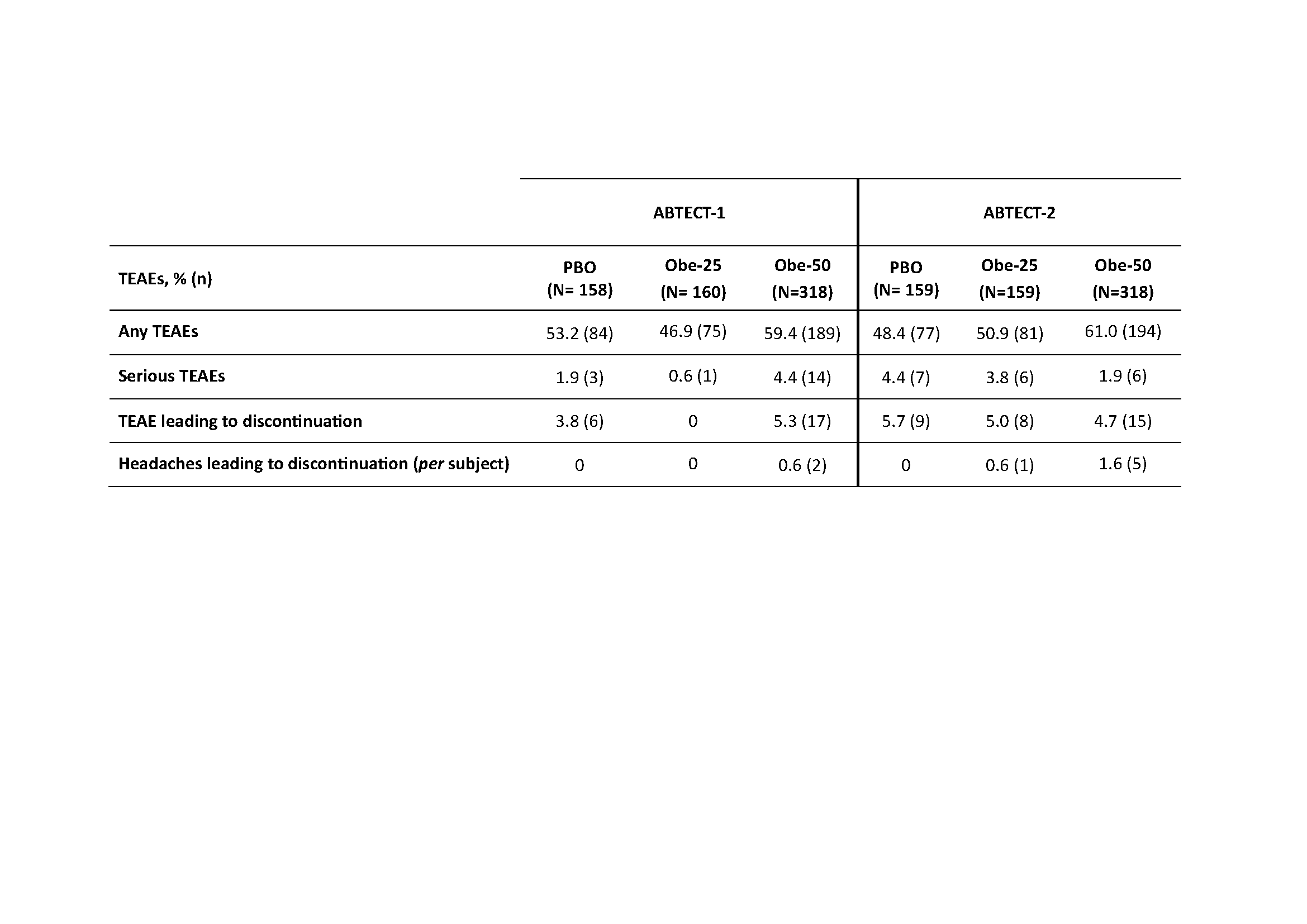
Results: 1272 pts were randomized and treated in ABTECT-1 (636) and ABTECT-2 (636). In both trials, baseline demographics and disease characteristics were similar between groups; 45.3% and 49.3% of pts had inadequate response to ≥ 1 advanced therapy. In both trials, a significantly higher proportion of pts receiving Obe-50 achieved clinical remission and all key secondary endpoints vs. PBO (Figure). In ABTECT-1, but not ABTECT-2, a significantly higher proportion of pts receiving Obe-25 achieved clinical remission and all key secondary endpoints. In a pooled analysis, both Obe-50 and Obe-25 met all primary and secondary endpoints with nominal significance (Figure). The rate of serious adverse events and treatment emergent adverse events (TEAEs) leading to study drug discontinuation for Obe-treated pts were similar to PBO. Proportions of pts who reported at least one TEAE were higher for Obe-50 and similar for Obe-25 vs. PBO in both trials. Headache was the most frequent TEAE; they were mild, short in duration, and not a barrier to treatment as evidenced by a low discontinuation rate (Table). Discussion: In both ABTECT trials, Obe treatment led to statistically significant improvements in clinical, endoscopic, symptomatic, and combined endoscopic-histologic endpoints at week 8. Obe was well tolerated and the overall safety profile was similar to previous studies, with no new safety signals.
Vermeire et al JCC 2023, 1689-97
Figure: Efficacy results at week 8 - Primary and secondary endpoints, ABTECT-1 and -2, pooled analysis‡ [a] % Difference is for obefazimod minus placebo and is based on estimated common risk difference using the Mantel-Haenszel weights adjusting for the randomization stratification factors: inadequate response to advanced therapies (yes/no), Baseline oral corticosteroids usage (yes/no), and region (Japan/rest of world) [ABTECT-2 only]. P-values are two sided. [b] Because this is a pooled analysis, all p-values are nominal. [c] 25mg did not meet the primary endpoint at week 8 in ABTECT-2 in the FDA testing protocol, therefore p-values for key secondary endpoints for the 25mg arm in ABTECT 2 are nominal. NRI is used for subjects with missing outcomes at Week 8 and subjects reporting any IE prior to Week 8. Clinical remission is defined as SFS = 0 or 1, and RBS = 0 and MES = 0 or 1 (MES of 1 modified to exclude friability); Endoscopic improvement is defined as MES = 0 or 1 (MES of 1 modified to exclude friability). Clinical response is defined as a reduction from Baseline in MMS >= 2 points and a relative reduction from Baseline in MMS >= 30%, and a reduction from Baseline in RBS >= 1 point and/or RBS = 0 or 1. HEMI is defined as MES = 0 or 1 and Geboes Index score <3.1 Symptomatic remission is defined as RBS=0 and SFS= 0 or 1 †For FDA testing protocol, symptomatic remission was an “other secondary” endpoint, not multiplicity controlled * Endoscopic improvement/symptomatic remission were co-primary endpoints for the EMA protocol and were met by both doses in both trials ‡Hierarchical testing strategy was used starting with 50mg for the primary endpoint followed by the key secondary endpoints; the 25mg was subsequently tested for the primary endpoint followed by the key secondary endpoints.
Table: Treatment-emergent adverse events (TEAEs) throughout 8 weeks in ABTECT-1 and ABTECT-2 Phase 3 trials


.jpeg.jpg "Bruce E. Sands, MD, MS, FACG photo")